Black, American Indian, and Alaska Native (AI/AN) women are two to three times more likely to die from pregnancy-related causes than white women – and this disparity increases with age, researchers from the Centers for Disease Control and Prevention (CDC) report today in the Morbidity and Mortality Weekly Report (MMWR).

Most pregnancy-related deaths are preventable. Racial and ethnic disparities in pregnancy-related deaths have persisted over time.
Pregnancy-related deaths per 100,000 live births (the pregnancy-related mortality ratio or PRMR) for black and AI/AN women older than 30 was four to five times as high as it was for white women. Even in states with the lowest PRMRs and among women with higher levels of education, significant differences persist. These findings suggest that the disparity observed in pregnancy-related death for black and AI/AN women is a complex national problem.
“These disparities are devastating for families and communities and we must work to eliminate them,” said Emily Petersen, M.D., medical officer at CDC’s Division of Reproductive Health and lead author of the report. “There is an urgent need to identify and evaluate the complex factors contributing to these disparities and to design interventions that will reduce preventable pregnancy-related deaths.”
The CDC’s Pregnancy-Related Mortality Surveillance System (PMSS) defines a pregnancy-related death as the death of a woman during pregnancy or within one year of the end of pregnancy from a pregnancy complication; a chain of events initiated by pregnancy; or the aggravation of an unrelated condition by the physiologic effects of pregnancy.
Key findings: 2007-2016 national data on pregnancy-related mortality
The CDC study, based on analysis of national data on pregnancy-related mortality from 2007-2016, found that:
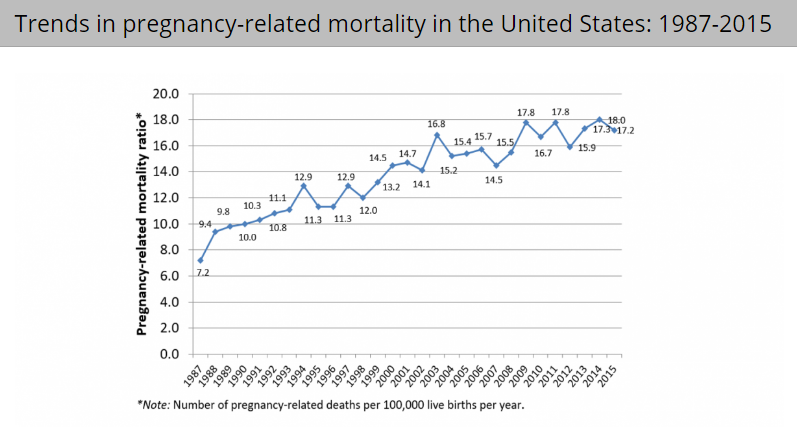
- Overall PRMRs increased from 15.0 to 17.0 pregnancy-related deaths per 100,000 births.
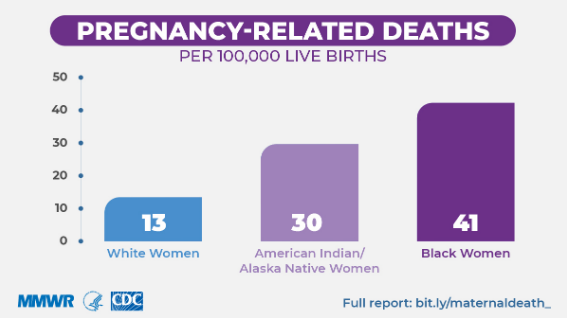
- Non-Hispanic black (black) and non-Hispanic American Indian/Alaska Native (AI/AN) women experienced higher PRMRs (40.8 and 29.7, respectively) than all other racial/ethnic populations (white PRMR was 12.7, Asian/ Pacific Islander PRMR was 13.5 and Hispanic PRMR was 11.5). This was 3.2 and 2.3 times higher than the PRMR for white women – and the gap widened among older age groups.
- For women over the age of 30, PRMR for black and AI/AN women was four to five times higher than it was for white women.
- The PRMR for black women with at least a college degree was 5.2 times that of their white counterparts.
- Cardiomyopathy, thrombotic pulmonary embolism, and hypertensive disorders of pregnancy contributed more to pregnancy-related deaths among black women than among white women.
- Hemorrhage and hypertensive disorders of pregnancy contributed more to pregnancy-related deaths among AI/AN women than white women.
- Disparities were persistent and did not change significantly between 2007-2008 and 2015-2016.
Reducing disparities in pregnancy-related mortality
Reducing disparities will require the participation of multiple systems to address the factors affecting these disparities.
Hospitals and healthcare systems can:
- Implement standardized protocols in quality improvement initiatives, especially among facilities that serve disproportionately affected communities.
- Identify and address implicit bias in healthcare that would likely improve patient-provider interactions, health communication, and health outcomes.
State and local Maternal Mortality Review Committees (MMRCs)offer the best opportunity for further identifying priority strategies that will reduce disparities in pregnancy-related mortality.





Crime & Safety
GBI Arrests Former Pearson Police Department Chief for Theft

Chattooga Local Government
Kennedy, Collins, Shaheen, Warnock introduce bill to cap cost of insulin at $35 per month

Chattooga Schools
GNTC student overcomes challenges through Accelerated Career program

Bulloch Public Safety
03/25/2026 Booking Report for Bulloch County
Bulloch Public Safety
03/09/2026 Booking Report for Bulloch County
Bulloch Public Safety
03/02/2026 Booking Report for Bulloch County
Bulloch Public Safety
03/16/2026 Booking Report for Bulloch County
Bulloch Public Safety
02/27/2026 Booking Report for Bulloch County
Bulloch Public Safety
03/10/2026 Booking Report for Bulloch County